



Z.14: ‘Operator Syndrome’?


I first heard about ‘Operator Syndrome’ when it was included in the House version of the 2025 National Defense Authorization Act (NDAA).
‘Section 732—Study on Testosterone Levels of Members of Army Special Operations Forces: This section would direct the Under Secretary of Defense for Personnel and Readiness to conduct a 5-year study on the impact of trainings and deployments on special forces' testosterone levels, and the potential repercussions to readiness and long-term health.’
The operator syndrome rider didn’t survive reconciliation with the Senate and ultimately wasn’t included in the final NDAA. If it had, the Secretary of Defense would have had to brief members of congress this year on available treatments for low testosterone in the military health system and current protocols for testing and screening. The briefing was to look closely at how ‘high-stress operating environments are linked to low testosterone’.
The NDAA wasn’t the first time I’d heard testosterone raised as a potential problem for soldiers. As I mentioned in G.9: Getting Older, several of my peers at the pre-command course last year claimed testosterone, or ‘low-t’, was the cause of their declining fitness.

Most recently, when I raised my concern about the negative consequences of steroid culture in our formations, a reader commented that we needed to relook steroids, raising operator syndrome as a justification:
The Army says the total testosterone levels in healthy adult males range from 300 to 1000 ng/dL (10.4015 to 34.6717 nmol/L).1 We have folks in our formation with testosterone levels in the low 300 range and we are telling them to drive on. By now, we have all heard of operators syndrome, and we know it’s killing us.

I didn’t ‘know it was killing us’, so I decided to look into it and see what I could find out. Spoiler alert: not much.
Now I’ll caveat this post. I’m far from even a novice in medicine and there may also be more research out there. My cursory search didn’t find it, but I’m open to other articles and studies if anyone has any. Feel free to comment, DM me, or email me with and studies or data you find out there.
Principally, the issue at hand seems to be where one draws a line on low-t. The reason this is a Downrange Data post is because I think it offers an example of the value of data literacy. When you’re working with data, it can often be more useful to draw curved lines than straight ones.
But I’m getting ahead of myself. First, to the research!2
Frueh, et al. The International Journal of Psychiatry in Medicine
Dr. Christopher Frueh has gone on to write a book, but the original 2020 article, ‘”Operator syndrome”: A unique constellation of medical and behavioral health-care needs of military special operation forces’ is the foundation of the work. It’s also the article most commonly cited in other articles I found referencing operator syndrome. Frueh and his eight co-authors lay out a constellation of issues they see as concomitant with life in special operations:3
interrelated health and functional impairments including traumatic brain injury effects; endocrine dysfunction; sleep disturbance; obstructive sleep apnea; chronic joint/back pain, orthopedic problems, and headaches; substance abuse; depression and suicide; anger; worry, rumination, and stress reactivity; marital, family, and community dysfunction; problems with sexual health and intimacy; being “on guard” or hyper vigilant; memory, concentration, and cognitive impairments; vestibular and vision impairments; challenges of the transition from military to civilian life; and common existential issues.
This is based off consultations with ‘…over 50 special operation forces operators (and many spouses or girlfriends) over the past 6 years’. So what we have is a small (n=50ish) initial qualitative study. This does not automatically undercut Frueh and his team’s work. A lot of scientific research starts with small qualitative studies. These can be the critical first step in identifying a trend, which leads to further studies, in particular quantitative ones.
Frueh argues that while lots of veterans struggle with PTSD and other challenges post-deployment, Special Operations Forces (SOF) is different ‘because of the unique and extreme nature of their military service’ and thus operators ‘are likely not well served by current programs or traditional models of care’.
Now who is and is not an ‘operator’ is an old debate, and not one I’m eager to jump into. It is one that any future qualitative study of operator syndrome will need to wrestle with though. Frueh specifically cites the below units:
Army (Green Berets, Rangers, Delta, and other special mission units [SMUs]); Navy (Sea Air and Land Teams [SEALS] and Special Warfare Combatant-Craft Crewmen); Marines (Marine Corps Forces Special Operations Command [MARSOC] and Force Recon); Air Force (Special Operation Squadrons, Combat Controllers, and Pararescue[PJs]); and explosive ordinance and demolition personnel who serve across branches. There are also personnel from other military and intelligence agencies (e.g., Central Intelligence Agency) who train and deploy with SOF.
This definition excludes Psychological Operations and Civil Affairs — who undergo their own selection — and many of the support soldiers who are assigned to these units, who are not always selected. Future studies could examine these populations to see what the divide is. The Rangers could provide an interesting pool to study since:
soldiers move into and out of the Ranger Regiment throughout their career and could potentially identify fluctuations over time.
like most SMUs, Rangers select all their support soldiers, which could provide another population to compare with non-selected support soldiers in other SOF units.
To be clear, when I use ‘Rangers’ I mean the the Ranger Regiment or ‘scrolled rangers’, not Ranger School graduates or ‘tabbed rangers’. This distinction will come up later.
Frueh proceeds to identify a list of challenges and potential causes for operator syndrome. And he lays out a great case for the impacts of Traumatic Brain Injury (TBI), which is where the paper is on its firmest footing. SOCOM is already studying the impact and ways to mitigate TBI. This is in no small part because ‘anecdotal estimates suggest 85% of SOF operators experience TBI from training alone.’ TBI can have dramatic and varied impacts, though it is not clear that SOF suffers uniquely. Other MOSs like Field Artillery are just starting to come to terms with the impacts associated with high volumes over a career of firing large caliber weapons. Having served alongside tanks, I would not be surprised to learn tankers and armored infantry are in a similar state.
Frueh identifies TBI as a contributor to nearly every other operator syndrome symptom including sleep disturbance, sleep apnea, chronic joint and back pain, orthopedic problems, headaches, depression, suicide, anger issues, endocrine health, memory, and vision impairment. This concurs with a lot of other research, both qualitative and quantitative, about the impacts of TBI.
But, where’s the link to testosterone? That’s buried back in endnote 22. There’s just one single source. A small 2019 study on just 65 Navy Seals.
Jensen, et al. Steroids.
Doctor Andrew Jensen, along with four other authors, published their study on 65 Navy SEALs in 2019.4 Participants were between 21 and 51 years old, with a range of years of service and number of deployments.5

The striking finding in this paper was 28 members of the study group (43%) had what the researchers defined as ‘levels below the clinically defined threshold for low-testosterone syndrome (LTS)’ or less than 10.4 nmol/L.

A clearly defined level for low-t wasn’t something I could find sources on. As you can see from the chart above, the researchers opted to draw a straight cutline at 10.4 to separate the study into two groups. Their source does list 10.4 as a limit, but I found other sources that listed lower values. The Australian Family Physician offered up a flow chart which suggested 8 nmol/L was an alternate floor:

Alternatively, I was able to find a comprehensive meta-study from 2014 which gave me the distribution of testosterone levels in men across their lives. Looking at data from sixteen different studies of testosterone they amassed a sample size of 10,458 men. When they plotted all those scores they found a distribution which looks like this:
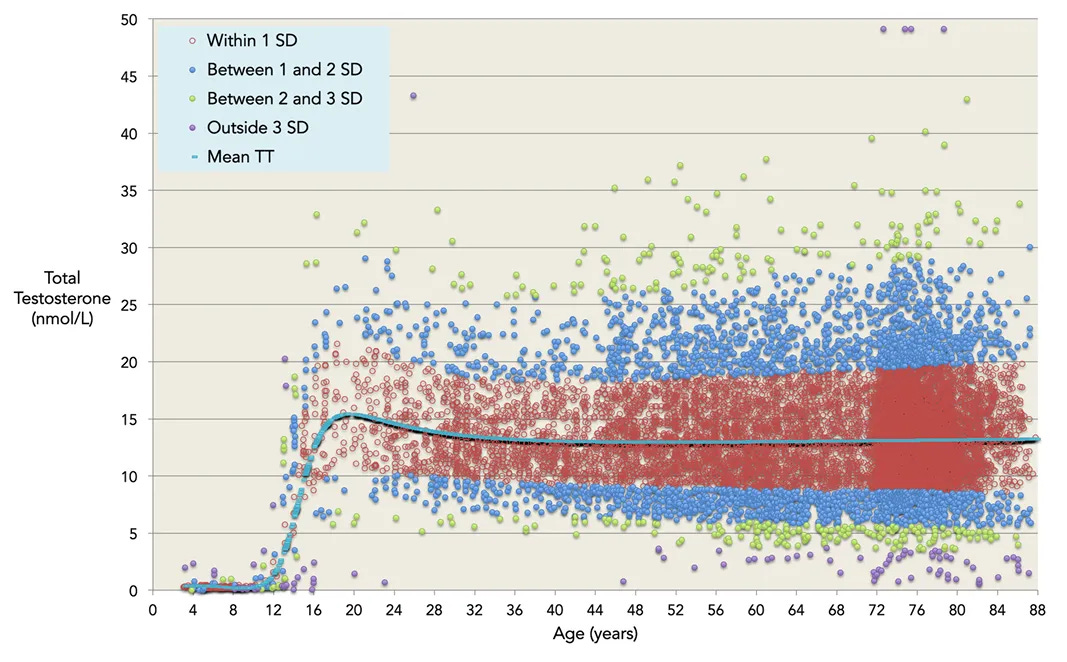
What I like about this dataset is it provides the distribution of scores instead of relying on an arbitrary cut-off score. It’s the normal curve vs. a carpenters straight edge. Being a single standard deviation (SD) outside the normal band is noteworthy, but not highly exceptional. I don’t have the individual data for each of the 65 SEALs in Jensen’s study, but they all land within this yellow box:

Right off the bat, one disparity jumps out to me. There is a lot more range on the high end than the low side. Jensen’s paper cites a normal total testosterone range from ‘10.4 to 41.6’. But according to the 2014 paper, which has a sample size 160.9 times larger, a nmol/L of 41.6 is somewhere between two and three standard deviations above the mean. It’s actually so abnormal, there’s not enough data in their larger data set to draw a clear dividing line between the two. According to the 2014 study, a normal range for that age group is closer to 18, which is not far from the 17.6 of Jensen’s mean for the non-low testosterone age group.
If we use the SDs from the 2014 paper instead of using the Jensen 10.4 cutline we get a distribution that looks roughly like this:

Some of the low-t group fits within the normal distribution, but without the raw data from Jensen it’s hard to pin down precisely how many. The bulk of the rest are only one SD below it, with a couple hitting two SDs below. On the upper end, we see about 11 SEALs who are one to two SDs above the normal distribution. It’s not a perfect bell curve of results, but it doesn’t look egregiously different than a random sample of males would. Indeed, the SEAL distribution mirrors the 2014 study’s distribution, with a narrower range of scores below the normal than above it.
Jensen and his co-authors didn’t cite any clear cause as to why these operators have lower testosterone. But they found no correlation between operator life and low-t:
Plasma testosterone concentrations were not correlated with age or time as an operator in our study.
Our data also show that the non-LT subjects exhibited adaptations that would provide enhanced resiliency to the normal stress response. This is made evident due to the positive correlation between cortisol and testosterone in the non-LT group… To add to this unanticipated finding, comparisons between the oldest subjects (≥35yrs) and the youngest subjects (<35yrs) failed to demonstrate any differences in any of the hormones measured. In fact, the oldest subject (51 yrs of age;> 30 yrs of service; 12 deployments) had total testosterone (12.5nmol · L−1) and all other measured hormones fell within the normal range for an adult male. [emphasis added]
Jensen concedes there are multiple causes for hormonal imbalances, including improper nutrition:
a typical Western diet that is high in fat intake leads to an increase in circulating sex hormone binding globulin, which limits the amount of biologically active testosterone circulating in the body.
23 of the SEALs kept a food log which was analyzed for macro and micro-nutrient content. The study calculated on average the SEALs were expending 3,382 kcals a day while consuming only 2,587.8, for a net -813.1 kcals per day — a 24% deficit compared to what they were burning. This seems to indicate their dietary intake was not the one they typically live off, but the researchers did not expound on it. They did find their low-t group had a 28.8% higher protein / fat macronutrient ratio than the non low-t group. As they cite in the article:
Other correlative and experimental studies have shown that a diet with a high PRO/CHO macro nutrient ratio depresses testosterone levels.
However, they go on to state:
Interestingly, unlike other studies our results indicate that dietary fat composition is not influential on testosterone levels. It is possible that the differences observed between studies are due to variations in physical training workload of the subject populations.
Without the raw data, I can’t investigate this assertion much. However, the physical training workload brings me to one mistake the researchers made in their paper.
Jensen’s team acknowledges that intense physical training and inadequate nutrition can temporarily reduce testosterone. They cite a study done on students completing Ranger School which found, ‘a significant decrease in circulating testosterone to the point that the average for all subjects was below the threshold for LTS’. The mistake is when Jensen goes on to conflate Ranger School with Ranger Regiment training:
The participants in our study were a cross sectional sample of elite naval operators, with daily training regimens that are similar to those of the Army Rangers; however, the subjects in our study had already completed on average 7.7 ± 0.9 years of elite military training, which is much longer than the 8-week long selection course completed in the Army Ranger studies.
So, there’s a huge difference between the daily training regiments of Army Rangers (scrolled) and the ‘8-weeks’ — if you’re lucky — of training in Ranger School (tabbed). I’m sure the level of training across all of Frueh’s operator teams is intense and physical, regardless of tribe. But as a graduate of Ranger School and two selections, I can attest that Ranger School takes a very different toll on your body. The ‘daily training regimens’ the SEALs were conducting are not the same.
This is principally because, unlike all those training events and other selections, Ranger school is the only one that starves you. Back in 2003 when I graduated Ranger school, I was almost 30 pounds (13.6 kgs) lighter than when I started because for most of course I was subsisting off a single meal per day. Ranger school is still a very physically demanding course, but it is highly likely starvation is the leading cause for students' testosterone dropping in the course. Regardless, as the Ranger School study found, ‘testosterone levels rebounded to pre-training levels within 2–6 weeks of the training stimulus removal’.6
Jensen’s team grant their initial study has limitations, the principle one being it only captures a single point in the operator’s career.
It fails to indicate whether or not individuals had pre-existing LT prior to service.
If SOCOM wants to collect the data it would not be very difficult. In keeping with last week’s post, SOF operators are already subjected to extensive physicals before they can even attend a selection event; adding in testosterone testing could provide baselines. Currently, testosterone levels are not part of these physicals, but there’s barely any cost in one more blood draw.

Additionally, while many operators undergo semi-regular medical screenings, there is a smaller subset of them who have to undergo regular detailed physicals. Military Freefall and Dive qualified operators have to redo their physicals every five years. These are the most thorough health screenings I have had and would provide SOCOM an easy pool of certainly more than 650 operators to gather data from at barely any extra effort. This would be 10 times the Jensen data set and would canvas across all the SOF tribes, not just west coast SEALs.
More Data, Less Snakeoil
I’m not arguing that operator syndrome is not a thing. But I do think it needs more data before people can confidently claim it is ‘killing us’. Jensen and his team concede as much in their article. Which, to reiterate, was the lone citation about operator testosterone Frueh offered in his 2020 article. Frueh didn’t even test the testosterone levels of the subjects of his study.
So it’s not clear why Frueh chose to make the following brazen claim when he spoke with Task & Purpose and said 'By 35 years old, many special operators have the same testosterone levels of 80-to-90-year-old men.’ This is nowhere in his paper, nor in Jensen’s.
It is, ironically, in the 2014 Kelsey study I found, but that’s because after around age 24, it doesn’t appear that men’s testosterone drops off as significantly as reported. Instead they found, ‘an increased variation in total testosterone levels with advancing age after age 40 years’.

In the same vein, the AWC’s s Maximizing Senior Leader Health and Wellbeing found that most military leaders don’t have clinically low testosterone. Instead, they found those with just reduced testosterone should reexamine their lifestyle. Overwhelmingly it was a sedentary lifestyle which led to an increase in unhealthy levels of fat stores and reduced t-levels. While not clinically low-t, these officers could restart their own natural testosterone production by engaging in a better fitness regime, in particular one that forgoes long, repetitive cardiovascular training. Instead, soldiers should focus more on higher intensity workouts that move weight as they age.
Diet is just one thing that soldiers could be putting into their bodies that reduces their testosterone levels. If we take another look at that flow chat from the Australian Family Physician, we see:

While we don’t know what the current usage rate of steroids in SOF is, we do know it’s not zero.
The Navy will begin randomly testing its special operations forces for steroids and other performance-enhancing drugs beginning in November, taking a groundbreaking step that military leaders have long resisted. - PBS Newshour
Further study might determine there is an operator syndrome, though for now I think the science points much more reliably to the impacts of TBI. Discussing the Houses’ call for the study, Rep. Jimmy Panetta (D-CA) stated, ‘Despite surveys of both veterans and active duty servicemembers indicating a potential link between the stress of military service and decreased testosterone levels, we still lack comprehensive data on this issue.’
He’s right, even if he doesn’t want to be. There’s a dearth of data to back up the ‘Operator syndrome’ concept. It doesn’t mean it’s wrong, but it means it needs more data and study before service members jump both feet into the idea that testosterone is the problem and the solution.
Unfortunately, I’m not sure calls for more data will resonate much these days. Our country seems to be in love with ‘win the internet’ content that has no science to back it up. As a nation we are opting more and more to support social media snake oil peddlers who will sell us supplements and Himalayan pink sea salt instead of data driven health decisions. Blatant AI generated slop isn’t ‘formatting issues’, it’s us lying to ourselves.
I’ve been advocating for more data literate leaders for over a year now, but in a world where data itself doesn’t matter, literacy isn’t even an option.
I’m converting all measurements into nmol/L to baseline with the two studies I reference later. Feel free to check my math here.
What little medical knowledge I do have has been heavily impacted by Aaron Carroll and his YouTube channel Healthcare Triage. ‘To the research!’ is his tag-line. I also highly endorse his book Bad Food Bible. While it provides a good overview of the current science of healthy eating, it is also a great primer on data literacy and how to read medical news.
I’m just going to use his name from now on, because ‘et al’ is going to get old, plus he’s the one who went on to sell a book.
Hereafter just Jensen, as with Frueh.
Also, as I’ve written elsewhere, BMI is a really bad metric, one that is not a great indicator for anything. In the Jensen study only the lowest SEAL BMI scores are barely inside the bounds ‘healthy’. The overwhelming majority are classified as ‘overweight’ or ‘obese’, despite being presumably fit operators.

‘Stimulus removal’ is my new favorite way to describe someone getting out of Ranger School.
Perhaps “it’s killing us” was a bit hyperbolic. I appreciate the education and the work that went into this sir.
There's been a bit of research on firefighters, and I've known many on testosterone treatment regimens. Here's one study. https://www.iaff.org/wp-content/uploads/Kuehl-edit-Testosterone-Information-Document-2020-2.pdf